The State of the World’s Children 2023: For every child, vaccination
Regional Brief: Europe and Central Asia

For every child, vaccination
Immunization is one of humanity’s most remarkable success stories. It has saved countless lives. Many more lives will be saved if the goals of the Immunization Agenda 2030 are achieved. This global strategy aims for a world where “everyone, everywhere, at every age, fully benefits from vaccines for good health and well-being”.
Immunization allows children everywhere to live lives free of many forms of disability and illness. It has led to the eradication of smallpox, a disfiguring and often fatal disease that in the 20th century alone claimed an estimated 300 million lives. There has been remarkable progress, too, in eradicating polio. The power of immunization was demonstrated again in the COVID-19 pandemic. The disease claimed 14.9 million lives – directly and indirectly – in 2020 and 2021, according to the World Health Organization (WHO), and disrupted lives around the world, especially children’s. While it has taken far too long to get COVID-19 vaccines to people living in the poorest countries, the global impact is still astounding: Already, at least two thirds of the world’s population has been immunized against COVID-19. Those vaccines have prevented an estimated 20 million deaths globally. These examples demonstrate that public demand, scientific innovations and – perhaps above all – political will can drive rapid change.
We must do more, and we must do better, now
Globally, an estimated 67 million children missed out entirely or partially on routine immunization from 2019 to 2021. In Europe and Central Asia, this figure is 931,000 children.1 As these children pass the age when vaccines are routinely given, it will require a dedicated effort to ensure that they catch up with their vaccinations.
The pandemic also exposed – and exacerbated – persistent weaknesses in health systems and primary health care. Key resources were diverted to respond to the pandemic, which, along with many other factors, contributed to the backsliding in routine immunization. But even before the pandemic, far too many primary health-care systems suffered from insufficient number of skilled health workers, especially in rural areas, limited access to essential supplies and equipment, weak capacity for collecting and using data and conducting disease surveillance, shortages at the local level of key medicines and vaccines, and barriers to using available resources efficiently and effectively.
In Europe and Central Asia, vaccine hesitancy is also a challenge. Attitudes on vaccines are influenced by people’s concerns related to vaccine safety, myths and misconceptions. Vaccine misinformation is often disseminated through traditional and social media, and anti-vaccination movements. Decreasing trust in the health systems also influences negative attitudes towards vaccine uptake.
1. This number is calculated based on the number of children who missed DTP1 and DTP3. See Box 1 for reference.
The consequences of failure
Unfortunately, the world continues to see far too many outbreaks of vaccine-preventable diseases. The consequences of failing to vaccinate children may become more severe in years to come. Climate change risks exposing new communities to infectious diseases, such as malaria, dengue and cholera and may alter seasonal disease patterns. Also of long-term concern is the rise of drug-resistant infections. Failure to immunize children sets back still further the prospects of attaining the Sustainable Development Goals (SDGs). Immunization is key to achieving SDG 3, which aims to “ensure healthy lives and promote well-being for all at all ages”. But it is also linked to 13 of the other SDGs. In that sense, immunization is at the heart of our collective commitment to achieve a better and more sustainable future for us all.
A time for political will
Much will have to happen if we are to protect every child against vaccine-preventable diseases. The needs are complex, even daunting. But overriding them all is one single necessity: political will. Nothing will happen unless we garner the political will – globally, nationally and locally – to protect children against vaccine-preventable diseases.
That will should be grounded in optimism. The emergence of mass immunization in the 1980s and the development of COVID-19 vaccines show we can make progress, and we can make progress quickly. Encouragingly, and despite the setbacks it caused to childhood immunization, the pandemic may also have helped lay the groundwork in some countries for faster progress.
Political will should also be grounded in the realization that immunizing children makes economic sense. At an average cost of about US$58 per child in low- and middle-income countries, the standard course of vaccines can contribute enormously to protecting against disease and lifelong disability. Despite shrinking national budgets in some countries, immunization must remain a priority because it is a proven strategy for reducing future health-care costs and supports economic growth. It generates strong returns on investment – as much as US$26 for every US$1 invested. Continued and sustainable investment in immunization as part of health budgets is essential. But governments and donors need to work together to improve the efficiency and effectiveness of planning, budgeting and service delivery.
Now is a time for determination.
Now is a time for political will.
Now is the time to protect the health of every child.
Immunization coverage in Europe and Central Asia
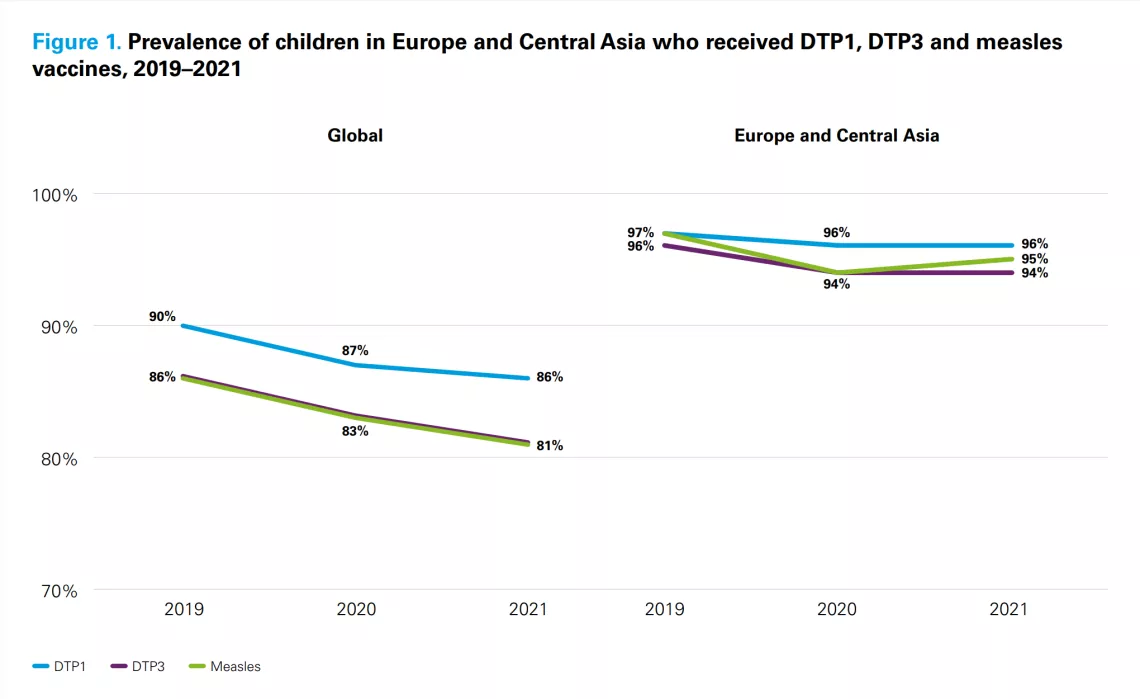
Europe and Central Asia has the highest immunization coverage rates in the world. However, the pandemic set back immunization coverage. Between 2019 and 2021, the coverage of DTP and measles vaccines dropped. This led to an increase in the number of zero-dose and under-vaccinated children.

Box 1. Understanding zero-dose
‘Zero-dose’ and ‘under-vaccinated’ have become key concepts in explaining immunization coverage, in aligning global efforts to improve vaccine coverage, and for monitoring success. What do they mean?
Zero-dose refers to children who have not received any vaccinations. Most live in communities that experience multiple deprivations.
Under-vaccinated refers to children who have received some, but not all, of their recommended schedule of vaccinations.
To calculate the numbers of zero-dose and under-vaccinated children, a proxy measure is used. Children who have not received the first dose of diphtheria, tetanus and pertussis (DTP1) vaccine are described as zero-dose. Children who have received DTP1 but not the third dose (DTP3) are described as under-vaccinated. Children typically receive these vaccines in the first year of life. In general terms, therefore, where data for zero-dose and under-vaccinated children are presented in percentage terms, these numbers represent percentages of surviving infants (rather than the entire child population).
Case Study 1: Kyrgyzstan
Though her daughter, Aila, was first vaccinated shortly after birth, Meerim Omurkanova hesitated when it was time for follow-up immunizations.
“I read on the internet that vaccinations could cause cerebral palsy and autism,” Omurkanova said. “And because of this, I initially did not want her to receive vaccinations.”
The internet misinformation – thoroughly disproven – ultimately fell apart under the influence of a much more respected source: Mirlan Dezhyusubekov, the imam of the mosque in Kaiyrma village, where Omurkanova and her family live.
“From a religious point of view, we cannot judge parents’ decisions to vaccinate or not to vaccinate their children,” Dezhyusubekov said. “But I tell families that I was vaccinated, as well as my children, and we have all been well.”
Misunderstanding and a lack of confidence in vaccination has been a concern in Kyrgyzstan, where the Republican Immunoprophilaxis Centre has received a growing number of reports of vaccination refusals since 2016. In 2021, there were more than 10,000 refusals. In addition, the number of infants in Kyrgyzstan who received a third dose of a vaccine against diptheria, tetanus and pertussis (DTP 3) fell in 2020 to 87 per cent, from 95 per cent in 2019 and 94 per cent in 2018.
An effort was launched throughout Kyrgyzstan to build confidence in vaccines and increase immunization coverage in 2019. The initiative focused on equipping volunteer Village Health Committees so they could coordinate with parents, caregivers, health-care professionals and religious leaders. Effective communication on immunization has helped change minds in communities throughout the country. In the Jayyl district, 164 of the 486 families who refused vaccination in 2022 changed their minds by the end of the year. In addition, UNICEF’s social mobilization efforts in four out of Kyrgyzstan’s seven provinces helped change the minds of thousands of parents and caregivers. In that time, more than 2,000 more children were immunized and entered into medical and national registries.
As a result of these efforts, Kyrgyzstan has a vibrant model of collaboration between parents, caregivers, medical workers, volunteers and religious leaders at the community level that can work to build and maintain trust in vaccination.




















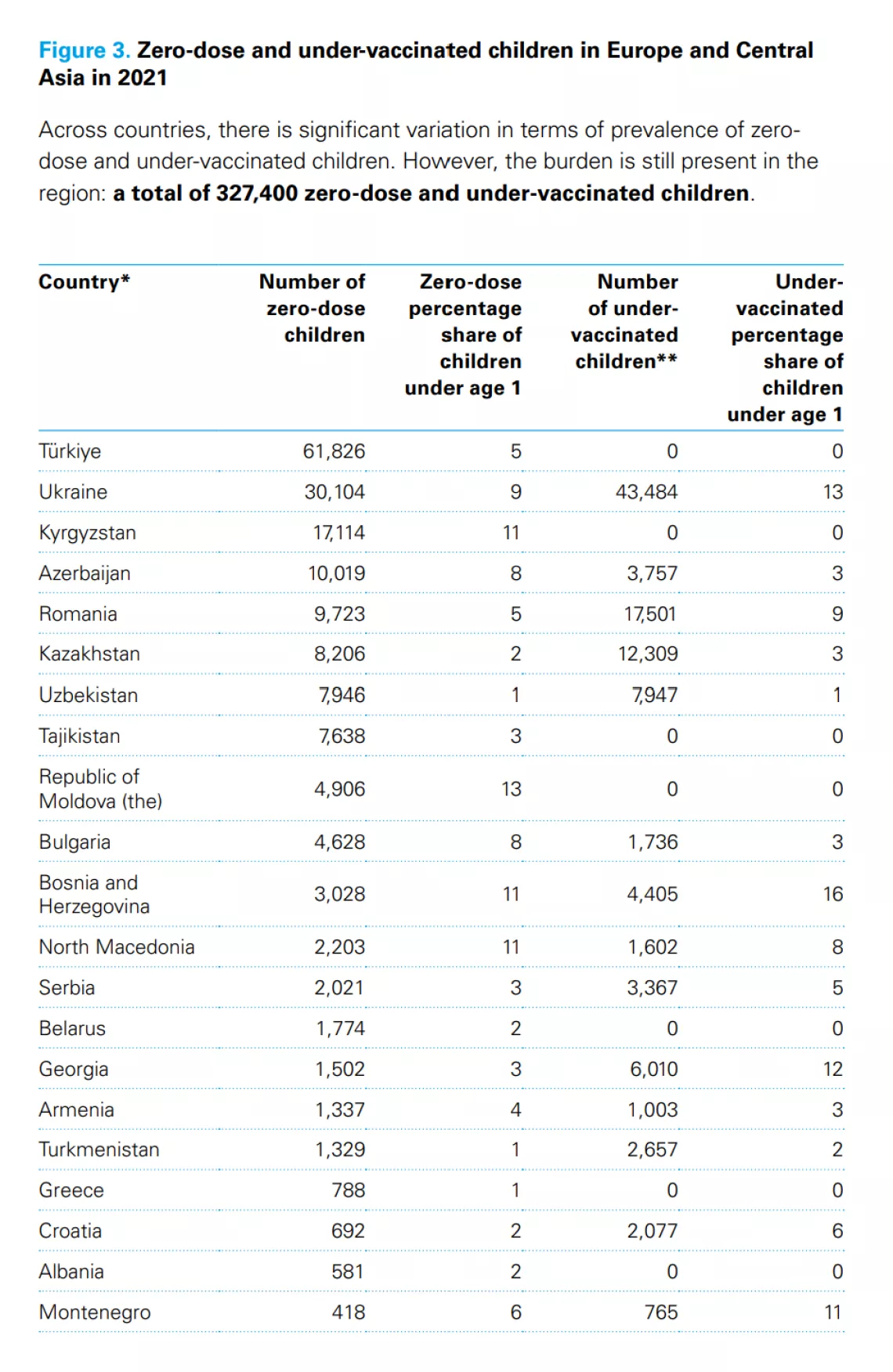
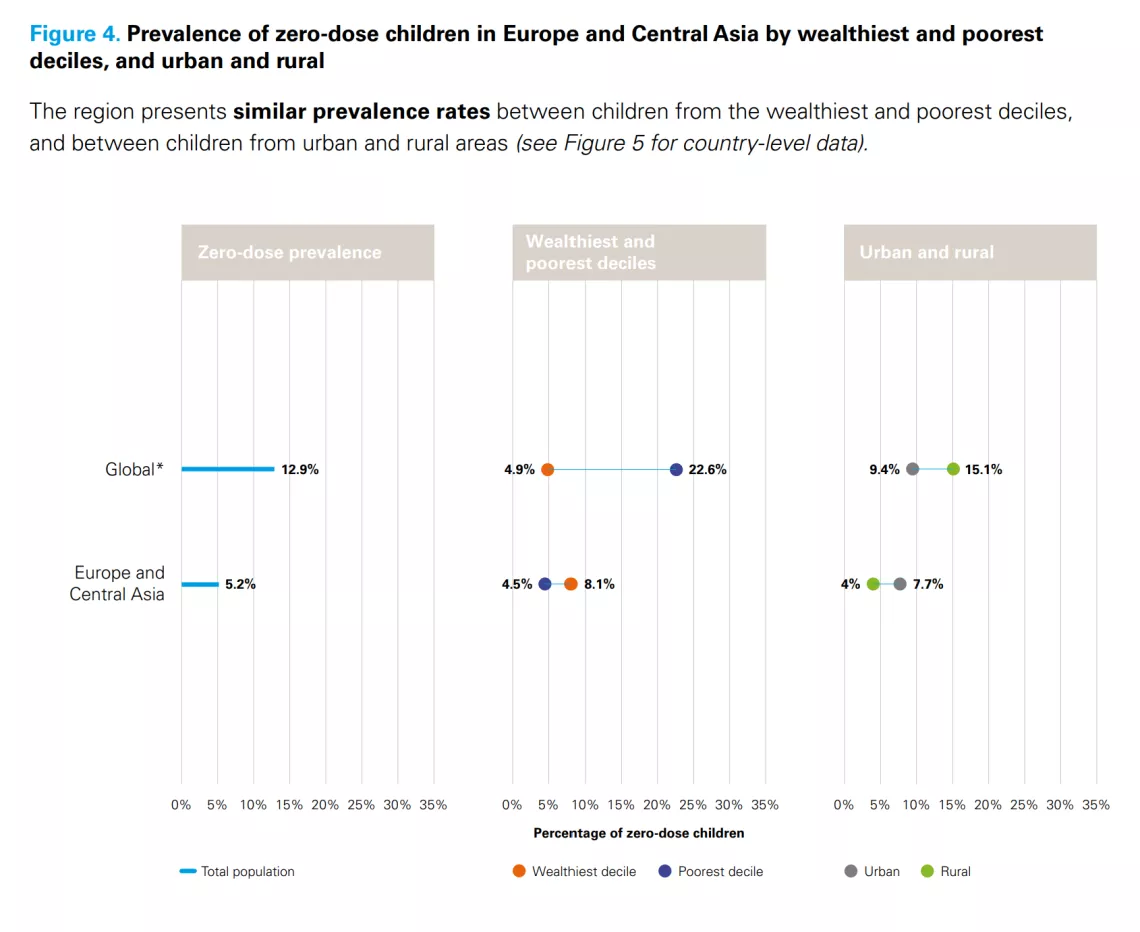
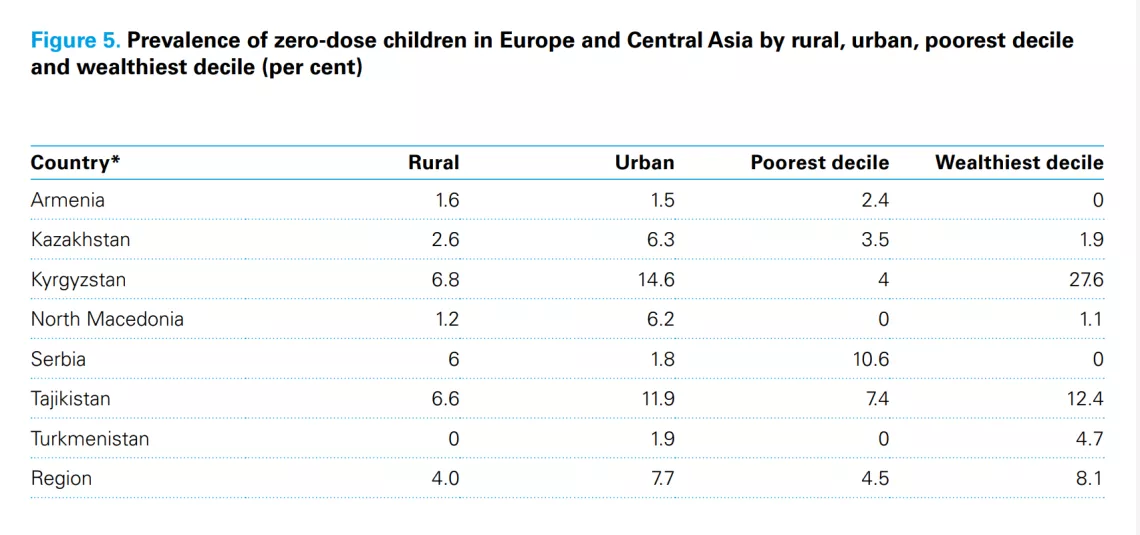
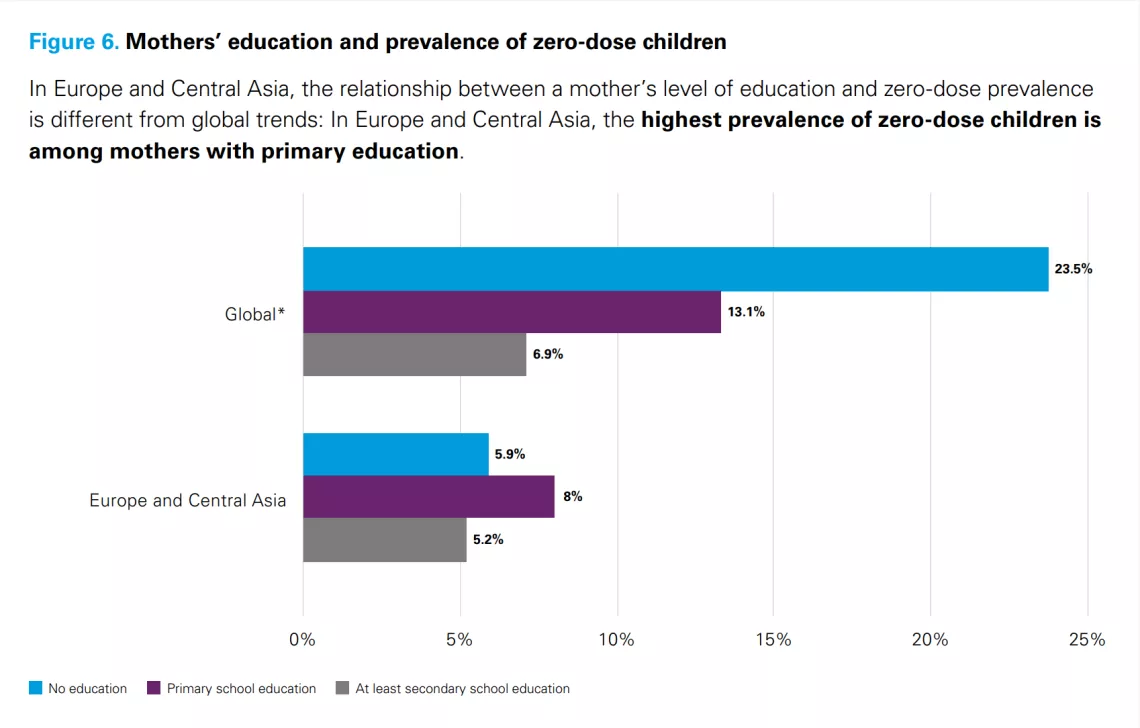
Who is missing out on vaccines?
An analysis for The State of the World’s Children 2023 shows some of the socioeconomic determinants associated with immunization.2 The numbers make the connection between children who miss out on vaccination and inequity. By global standards, Europe and Central Asia has low zero-dose prevalence.
2. This analysis includes surveys carried out from 2015 to 2020, covering 74 countries. The most recent Demographic and Health Surveys (DHS) and Multiple Indicator Cluster Surveys (MICS) from that period were included for each country.

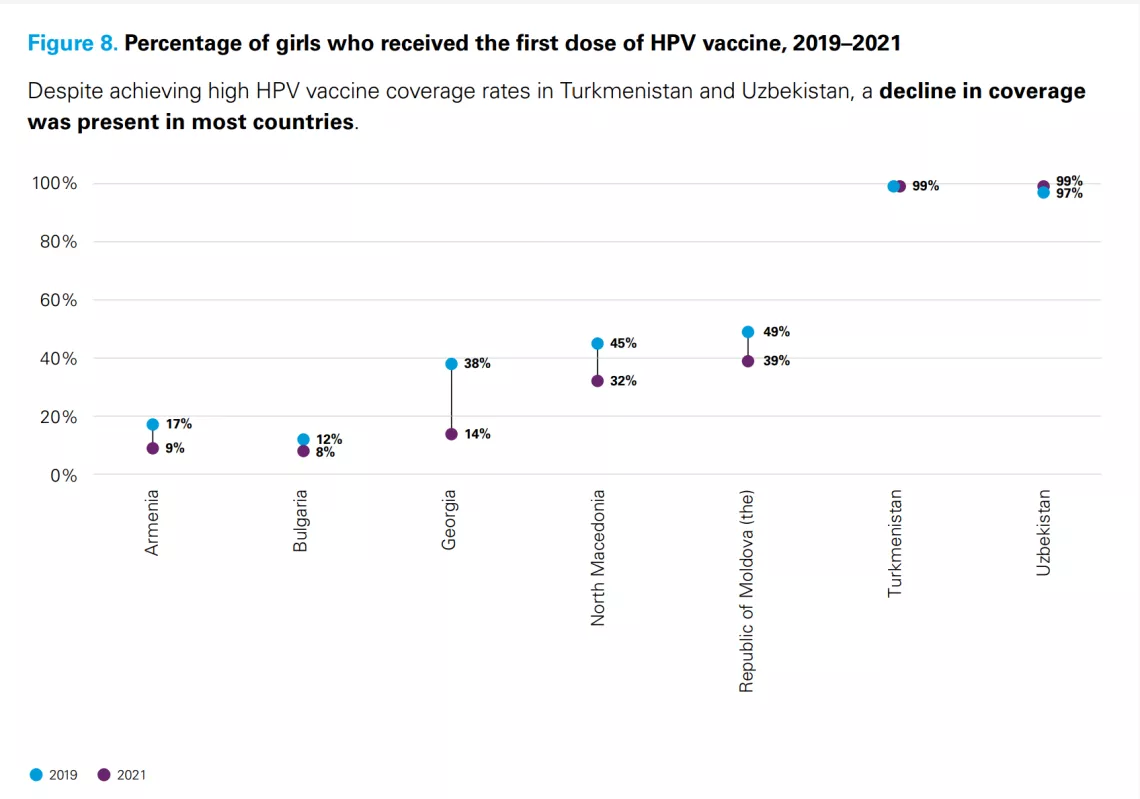
Adolescent girls’ health: Focus on HPV
According to the World Health Organization, more than 95 per cent of cervical cancer is caused by sexually transmitted human papillomavirus (HPV). The HPV vaccine helps protect against a number of cancers, notably cervical cancer, which is estimated to be the fourth largest cause of cancer deaths among women worldwide.
Case Study: Uzbekistan
At age 14, Shakhrizoda Alanazarova knows all too well the benefits of vaccination. Five years ago, she and her family lived through a stressful time when a close relative was diagnosed with cervical and breast cancer. Despite treatment, Shakhrizoda’s relative died at the age of 43. So, when the family health clinic introduced the new vaccine to protect against the virus that causes cervical cancer, Shakhrizoda and her family decided not to miss the opportunity.
“Cancer is a bad illness and ends badly,” Shakhrizoda said. “I want to stay healthy. I do not want my mother and father to worry.”
As Shakhrizoda and her family know from tragedy, cervical cancer can cause plenty of worry. It has been a concern for the Government of Uzbekistan as well.


Every year, more than 1,600 new cervical cancer cases are diagnosed, and about 850 women die of the disease. In response, the Government of Uzbekistan introduced the HPV vaccine in the national immunization calendar in 2015 and began implementation in 2019 with coverage that reached 98.6 per cent of eligible girls.
Since the HPV vaccination requires two doses, the second phase landed in the middle of the COVID-19 pandemic lockdowns: a potential challenge for the roll-out of the new vaccine, according to Dilorom Tursunova, Head of the Immunization Department and Expanded Programme on Immunization (EPI) at the Sanitary and Epidemiological Welfare and Public Health Service of the Ministry of Health.
Despite the concerns, the country persevered, and when the second doses were provided in June 2020, the coverage rate reached 97.8 per cent. Winning public trust for the vaccine was one of the biggest challenges, Tursunova said. Rumours linked the HPV vaccine with infertility. In response, the ministry and its partners launched a campaign on multiple media platforms that included tailored messages for parents and religious leaders, and endorsements from key influencers. In Uzbekistan, only girls aged 9–14 years are given the HPV vaccine. Like Shakhrizoda, many girls and their families received invitations from schools or local clinics.
“We did convince our population, after all,” Tursunova said.
Understanding behaviours to drive vaccine confidence
The UNICEF Regional Office for Europe and Central Asia is using an innovative process of behavioural insights (BI) to understand and identify barriers to immunization and address vaccine hesitancy.
BI is a field that draws on research from psychology, economics, sociology and neuroscience to generate insights about why people make the choices they do. It helps governments and international organizations design people-centred policies and programmes that consider the psychology of decision-making.
Considering the urgent need to increase timely childhood vaccination and address vaccine hesitancy, the UNICEF Regional Office for Europe and Central Asia, in collaboration with the UNICEF Office of Innovation and UNICEF Innocenti, is supporting Bosnia and Herzegovina, Georgia, Kyrgyzstan, Montenegro, North Macedonia and Uzbekistan to use BI to drive immunization uptake.
A standard BI approach includes five iterative phases: ‘Target’, ‘Explore’, ‘Solution’, ‘Implementation’ and ‘Evaluation’. The first phase involves identifying the target behaviour [i.e., timely measles, mumps and rubella (MMR) vaccination and population (i.e., eligible children aged 12–15 months)]. Evidence reviews and qualitative research identify specific barriers to immunization. Then, a participatory human-centred design approach is used to identify, pretest and refine relevant evidence-based behaviour change interventions that could be scaled up in each country’s context. The EAST and MINDSPACE frameworks (developed by Behavioural Insights Team) identify potential solutions with relevant stakeholders (e.g., caregivers, policymakers and health workers). Once pretests are finalized, the solutions are then evaluated through appropriate methods to understand potential effectiveness in increasing vaccination.
The BI method is being applied in Montenegro, Bosnia and Herzegovina, and North Macedonia to increase MMR vaccination; in Kyrgyzstan to increase all vaccinations given to children aged 0–12 months; and in Georgia to increase HPV vaccination.
A framework for action
Despite undeniable progress over many decades, we continue to face critical challenges in immunization. Immunization coverage has fallen back, or stagnated, in too many places. We are persistently missing children with life-saving vaccines, especially the socially marginalized and poorest children, and the situation has only deteriorated during the pandemic. The failure of health systems to reach every child with vaccines reflects domestic underinvestment in primary health care, inadequate human resources for health, and leadership gaps across different government levels and areas.
The decline in immunization throughout the pandemic should sound an alarm bell: Routine immunization must be a priority in the coming years. We must take concerted action to catch up on children who missed out on being vaccinated during the pandemic, rebuild systems and tackle major gaps in health systems. Failure to act will devastate the lives of today’s children and adolescents and tomorrow’s adults, and will set back still further progress towards reaching the SDGs.
Building on the global strategies outlined in the Immunization Agenda 2030, European Immunization Strategy 2030 and the Gavi Strategy 5.0 to promote equity and sustainably scale up immunization coverage, presented here is a set of concrete and actionable recommendations to reach every child with vaccines and to ensure that immunization and primary health-care systems are ready to meet future challenges.
Enacting this agenda will require strong political will from governments and other major stakeholders in the immunization landscape. The COVID-19 pandemic has shown the centrality of collective and concerted action to ensure that vaccines reach everyone. We are constantly reminded that “vaccines don’t save lives; vaccination saves lives”. For vaccination to happen, political will must be a number one priority across countries.
1. Vaccinate every child, everywhere
Vaccination is an equity agenda. This means reaching children who missed out on vaccination during the pandemic; children in remote locations, informal urban settlements and conflict areas; and zero-dose children.
Key priorities:
- Catch up on the vaccination of children missed during the pandemic: The COVID-19 pandemic response generated enormous momentum for immunization, which can now be used to focus on the needs of children who were not vaccinated over the last three years. Tailored responses are needed in the countries most affected, backed by financial and other support from key donors and international partners.
- Identify zero-dose and under-vaccinated children and address key inequities: Use high-quality and fit-for-purpose data to identify zero-dose and under-vaccinated children and to inform and guide action, and invest in new technologies and approaches to make data timelier and more granular. Develop an individual child-health record system to monitor outcomes, including a community’s vaccine status, and monitor progress and needs with publicly accessible dashboards. Design immunization services to be responsive to addressing key socioeconomic inequities and barriers to accessing immunization.
- Identify children in urban areas, and access children in rural areas: In urban areas, strengthen community engagement to encourage people to engage with health services; improve security for parents and health workers; and offer flexibly timed vaccine services. In rural areas, focus on motivating and retaining health workers with salary top-ups and other incentives; consider using private operators or mobile teams to lower the high marginal cost of delivering vaccine services; and better integrate health services across sectors.
- Meet the challenges in emergency and fragile settings: Invest in preparedness to ensure countries are equipped to respond, including through the creation of contingency stocks, resilience-building and civil society engagement. Support children and families on the move, ensuring vaccines and health services are available and accessible. Prioritize and invest in innovative solutions, such as using mobile money and digital systems to pay health workers and developing vaccines with longer shelf-lives.
2. Strengthen demand for – and confidence in – vaccination
Understanding factors that influence vaccine readiness with effective social listening is critical to identify and develop tailored interventions and strategies that can help promote vaccine demand. Demand for immunization should be mainstreamed into national health budgets to ensure sustainable funding for programmes and activities that promote demand for and confidence in vaccines.
Key priorities:
- Talk to communities: Strengthen engagement with communities to better understand their attitudes towards the safety of vaccines and the value of vaccination; their experiences – both good and bad – with health systems and government officials; and the support they need if they are to take the time to vaccinate their children.
- Tackle gender barriers: Use innovative approaches to inform and educate caregivers, especially mothers; involve and engage fathers and men; and tailor services to meet the needs of time-pressed caregivers.
- Equip health workers to address concerns: Health workers enjoy high levels of trust. They should be supported to be powerful allies to persuade parents to vaccinate children, counter misinformation in the community, and inform the design of responses that meet families’ needs.
- Rethink accountability in health systems to boost trust: Governments should consider setting up well-designed governance bodies, such as health-care facility committees, to give community leaders a formal mechanism for voicing concerns and tackling issues related to immunization and primary health-care services in their area.
3. Spend more and spend better in immunization and health
Despite significant global investment in immunization and health systems-strengthening, health systems in many countries remain fragile.
Key priorities:
- Invest in primary health care at the national level: Governments should prioritize funding for primary health care to ensure it does more to meet the needs of its users and ensures equitable access, especially to underserved communities.
- Better align donor support: Donors should work to integrate their support into national priorities and national systems, shifting from disease-specific initiatives to systems-strengthening. Better harmonization of support can help reduce fragmentation and eliminate wasteful overlaps, including the duplication of, among others, infrastructure, service delivery and information platforms.
- Strengthen leadership capacity and promote accountability: Improve mechanisms for social accountability to ensure transparency, adequate budget allocations, quality of service and community engagement. Such approaches should be part of an overall push to maximize returns on current investment by improving planning and budgeting, identifying budget challenges, improving public financing management systems, and strengthening coordination between national-level ministries and between national and subnational levels of government.
- Explore innovative financing: Stakeholders at all levels need to build on recent successes and explore how innovative financing mechanisms can maximize returns on current investment and tap into new sources of funding. Such approaches need to be informed by a clear understanding of the potential risks involved, as well as the need for governance and oversight.
4. Build resilient systems and shock-proof them for the future
Resilient systems can respond to outbreaks, epidemics or pandemics, while continuing to provide essential services.
Key priorities:
- Focus on health workers, especially women: Improve pay and working conditions to motivate and retain health workers. They need to be better represented in leadership; offered access to training and professional advancement; protected from discrimination; and provided with flexible working arrangements to help them better manage their family and professional commitments.
- Improve data collection and disease surveillance: Within broader information systems for primary health care, it is essential to improve data collection on immunization and ensure it is actionable. Countries also need to build and strengthen comprehensive surveillance systems for vaccine-preventable diseases as part of a national system for public health surveillance, all supported by strong and reliable laboratory networks.
- Secure vaccine and other supplies: Ensure a secure supply of high-quality vaccines and related commodities. Making better use of pooled procurement processes and strategies can ensure affordable prices and support strategic stockpiles. The potential of expanded regional manufacturing to speed up and diversify vaccine supplies also needs to be fully explored and supported.
- Develop and promote worthwhile innovations: Invest in novel delivery technologies, such as solar-powered cold chains, heat-resistant vaccines and micro-array patches, to ensure access to vaccines for communities in the most challenging settings. Digitalization of stock managements should also be prioritized to enable real time data and avoid stock outs.
Highlights
For every child, vaccination
Immunization is one of humanity’s most remarkable success stories. It has saved countless lives. Many more lives will be saved if the goals of the Immunization Agenda 2030 are achieved. This global strategy aims for a world where “everyone, everywhere, at every age, fully benefits from vaccines for good health and well-being”.